Master’s Thesis
Integrating Ketogenic Metabolic Therapies in the Prevention of Depression, Bipolar & Schizophrenia
A Public Health Framework — Master of Public Health thesis, The George Washington University.
June 10, 2024
Abstract
Purpose: Serious mental illnesses, major depression, bipolar disorder, and schizophrenia affect many people, families, and society, with over 11% of the U.S. adult population experiencing these illnesses in the past year. A 30% subset of this population is “treatment resistant” to traditional therapeutic methods. The purpose of this critical analysis is to identify and establish a framework for how ketogenic metabolic therapies can be integrated into healthcare and community settings to aid in the prevention of major depressive disorder, bipolar disorder, and schizophrenia in the U.S. population. Methods: A literature review was performed using PubMed and Scopus. Results: 157 full-text articles were assessed for eligibility, and 16 were included in the review. Articles included studies demonstrating ketogenic metabolic therapies' metabolic and psychiatric outcomes and studies testing supporting psychoeducational programs, behavior change strategies, and adherence tools. Conclusions: Evidence shows potential for a monumental change in mental health prevention and delivery. Metabolic health outcomes are related to the risk for and management of serious mental illnesses. We must be prepared for how new information, treatments, and programs will be integrated and what it means for public health. This analysis offers a framework based on the Social-Ecological Model to develop supporting strategies for individual, relationship, community, and societal factors at each level.
Background
Major depression, known as major depressive disorder (MDD), bipolar disorder (BD), and schizophrenia, are all serious mental illnesses that affect the mental health of many individual U.S. citizens.1 The impact of these conditions also extends into their relationship with families, local communities, and the societal public health of the United States.1
Defined by the Diagnostic and Statistical Manual of Mental Disorders (DSM-5), MDD is at least two weeks when a person experiences a depressed mood or loss of interest or pleasure in daily activities and has most of the specified symptoms, such as problems with sleep, eating, energy, concentration, or self-worth.2 The prevalence of MDD among adults in the United States is staggering; an estimated 21 million or 8.3% of the adult population aged 18 or older experienced at least one major depressive episode in 2021.3 Risk factors for MDD include a history of traumatic or stressful events, alcohol or drug abuse, a history of other mental health disorders, a serious or chronic illness, and a family history of mental illness or drug abuse.4
Schizophrenia is a complex mental disorder characterized by disruptions in thought processes, perceptions, emotional responsiveness, and social interactions.5 The exact causes of schizophrenia are unknown. Research suggests a combination of physical, genetic, psychological, and environmental factors can make a person more likely to develop the condition.6 Individuals at an increased risk of schizophrenia include those who have a family history of the condition; this has been seen in identical twin studies, whereas if a twin develops schizophrenia, the other twin has a 1 in 2 chance of also developing the condition.6 Estimates of the prevalence of schizophrenia and related psychotic disorders in the U.S. range between 0.25% and 0.64%.5
Bipolar disorder (BD) is characterized by dramatic shifts in mood, energy, and activity levels that affect a person’s ability to carry out day-to-day tasks.7An estimated 2.8% of U.S. adults had BD in the past year.7 An estimated 4.4% of U.S. adults experienced BD at some time in their lifetime.7Risk factors that increase the development of BD or act as a trigger for a first episode include a first-degree relative having BD, periods of high stress, or drug and alcohol abuse.8
Among this population of over 11% of U.S. adults who experienced these illnesses of MDD, BD, and schizophrenia in the past year 3,5,7 a large subset of individuals diagnosed with these serious mental illnesses are classified as “refractory” or “treatment-resistant”.9 Refractory patients are defined as those who haven't responded to at least two treatment trials with drugs from different pharmacological classes, each used in an adequate dose for a sufficient period.9 Treatment-resistant depression affects about 30% of people diagnosed with MDD,10 treatment- resistant schizophrenia occurs in approximately 30% of individuals diagnosed with schizophrenia,11 and up to 33% of bipolar patients are refractory to an adequate trial of therapeutic interventions.12
Eliciting new hope is an emerging field of “metabolic mental health,” showing a link between the metabolic health of individuals and their risks for serious mental illnesses such as MDD, BD, and schizophrenia.13 Metabolic psychiatry is a subspecialty of psychiatry focused on identifying the root causes of metabolic dysfunction and pioneering metabolic treatments to improve mental health outcomes.14 The term “metabolic psychiatry” was coined by Stanford University professor Dr. Shebani Sethi.14 This field delivers emerging evidence for using the ketogenic diet (KD) to target metabolic and mental health as a dietary intervention.13 These practices, called Ketogenic Metabolic Therapies (KMT), use the ketogenic diet as a high fat, moderate protein intake, and severe carbohydrate restriction, typically less than 20 grams of carbohydrates per day.15 This dietary intervention induces a state of nutritional ketosis, where cells switch from burning mainly sugar (glucose) as their primary energy source to burning mainly fat (fatty acids and ketones).15 This process generates ketone bodies, which serve as an adjunctive fuel source for the brain, reducing its dependence on glucose.15 A retrospective analysis, titled The Ketogenic Diet for Refractory Mental Illness: A Retrospective Analysis of 31 Inpatients, shows the efficacy of the ketogenic diet in this context. The study placed patients admitted to a psychiatric hospital on a ketogenic diet as an adjunct to conventional inpatient care.15 Of the 28 patients (MDD n=6, schizophrenia n=10, BD n=12) who finished the study, 43% of participants achieved clinical remission, 64% experienced a reduction in medication doses upon discharge, and 100% of individuals had symptomatic improvement following the implementation of the ketogenic diet alongside conventional care (Figure 1).15
This evidence pointing to a connection between altered metabolism and mental health disorders in the brain suggests that both individualized clinical treatment and population-level programs aimed at preventing the root of metabolic dysfunction have the potential to improve patient and population-level outcomes of serious mental illnesses.16 Research from Stanford Medicine suggests that developing a metabolic disorder such as insulin resistance can double your risk for depression, even if you have no prior history of mental illness.16
7 out of 8 adult Americans have poor metabolic health, defined by levels of the five traditional cardiometabolic risk factors.16 With even higher rates of poor metabolic health among those who suffer from psychiatric diseases,16 there is an extraordinary opportunity to improve the health of the U.S. adult population by reducing the prevalence of MDD, BD, and schizophrenia.
The preliminary findings of the ketogenic diet used as a dietary intervention for the treatment of MDD, schizophrenia, and BD show transformative potential not only for the individuals facing refractory serious mental illness but for practices of improving metabolic health, such as dietary interventions and actions to support the scalability of using diet as a modality of prevention and intervention, to be integrated into a U.S. public health approach to prevent the onset of these severe mental health conditions.
As this field continues to evolve, many steps and collaborative efforts are needed to strengthen and bring these new practices together with the current mental health landscape. The United States public health system encompasses a wide range of stakeholders, including all public, private, and voluntary entities that contribute to delivering essential public health services within the country.17 This includes vital continued research in the form of randomized control trials. Currently, there are more than a dozen clinical trials that are now completed or underway investigating the use of the ketogenic diet for serious mental illness conditions, including major depression, schizophrenia spectrum disorder, bipolar disorder, and anorexia.18 An integrated public health approach will also require a robust public health communication effort to inform, educate, and empower the public about new prevention and intervention methods for these conditions. In addition, a set of practices and recommendations such as screening tools, industry- standard operating procedures, and program planning with community partnerships will be critical to a well-rounded public health approach. The evidence around the ketogenic diet to address MDD, BD, and schizophrenia is still growing. However, the public health field will benefit by having a proactive framework for adapting this innovative approach to healthcare settings. With that perspective, there will need to be federal, state, and local practices and policies addressing 1) enabling insurance reimbursement for interventions, 2) educating and maintaining a trained workforce, 3) evaluating the sustainability and quality of our food system, 4) encouraging the use of HSA/FSA accounts to fund preventative services and products; and 5) establishing laws and safety measures to support providers, individual health, and the promotion of public health.
Specific Aims
This critical analysis aims to identify how metabolic mental health research and interventions, such as ketogenic metabolic therapies, can be integrated into healthcare and community settings on a population level to aid in the prevention of MDD, BD, and schizophrenia in the U.S. population. A second aim is to establish a framework of strategies and recommendations for how providers, public health professionals, and health policies can work together to advance the knowledge and integration of the ketogenic diet as a dietary intervention in the prevention and treatment of MDD, schizophrenia, and BD to improve public health.
Methods
A comprehensive literature review was conducted in April 2024 to collect, organize, aggregate, and analyze literature related to the use of ketogenic metabolic therapies as a dietary intervention in the treatment of MDD, schizophrenia, and BD. The literature review investigated the gaps, opportunities, and precedence in the current landscape for implementing this novel treatment and supporting programs and what public health implications it will have.
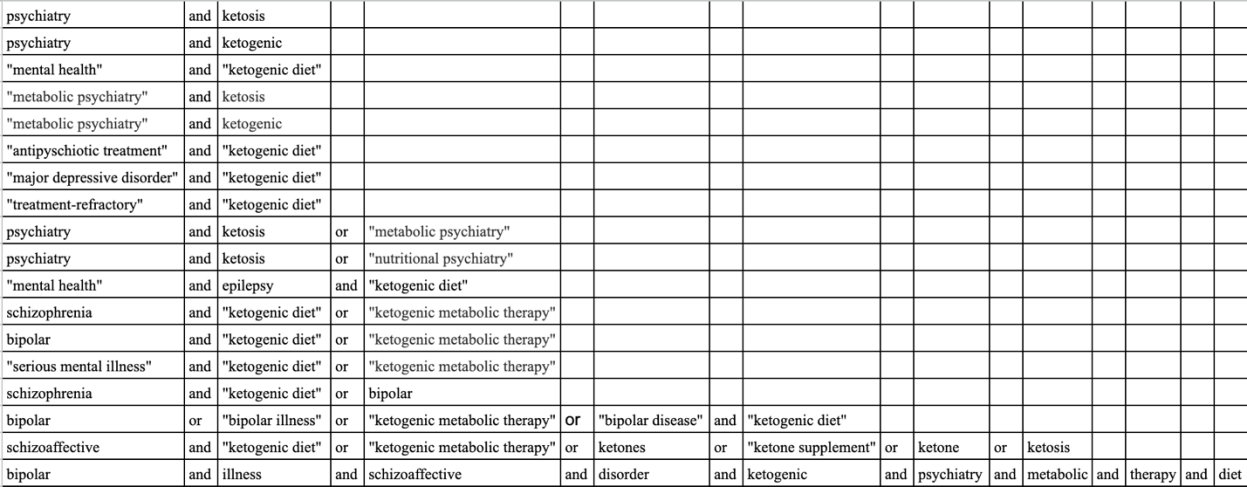
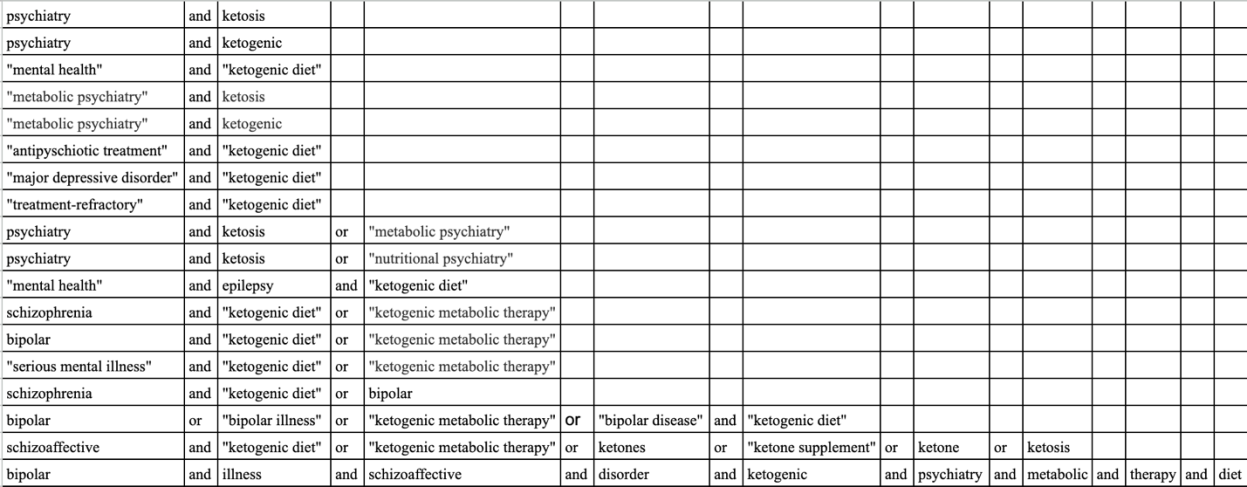
Scopus and PubMed were used as databases to search. Unique search terms were used, including “mental health,” “ketogenic metabolic therapy,” “metabolic psychiatry,” “ketogenic diet,” “treatment-refractory,” “serious mental illness,” “schizophrenia,” “bipolar,” “major depressive disorder,” “epilepsy,” and additional related terms were used to collect literature. A full table of the search terms and combinations used can be seen in Figure 2 of the appendix. The literature was compiled, organized, and analyzed using the systematic review management software Covidence for relevant inclusion and exclusion criteria. Studies focused solely on children or infants ages 17 and under were excluded. International research was included to contribute to scientific rigor. However, the analysis focuses on U.S. citizens and the implications for U.S. public health.
Extensive research exists on the ketogenic diet as a treatment modality for stopping seizures in epilepsy. Because the ketogenic diet has a history of medical efficacy for epilepsy, literature discussing evidence and practice guidelines for the ketogenic diet as a treatment for epilepsy was included as examples and references for the precedence of a successful dietary intervention in medical treatments. Research published before 2014 was excluded.
Results
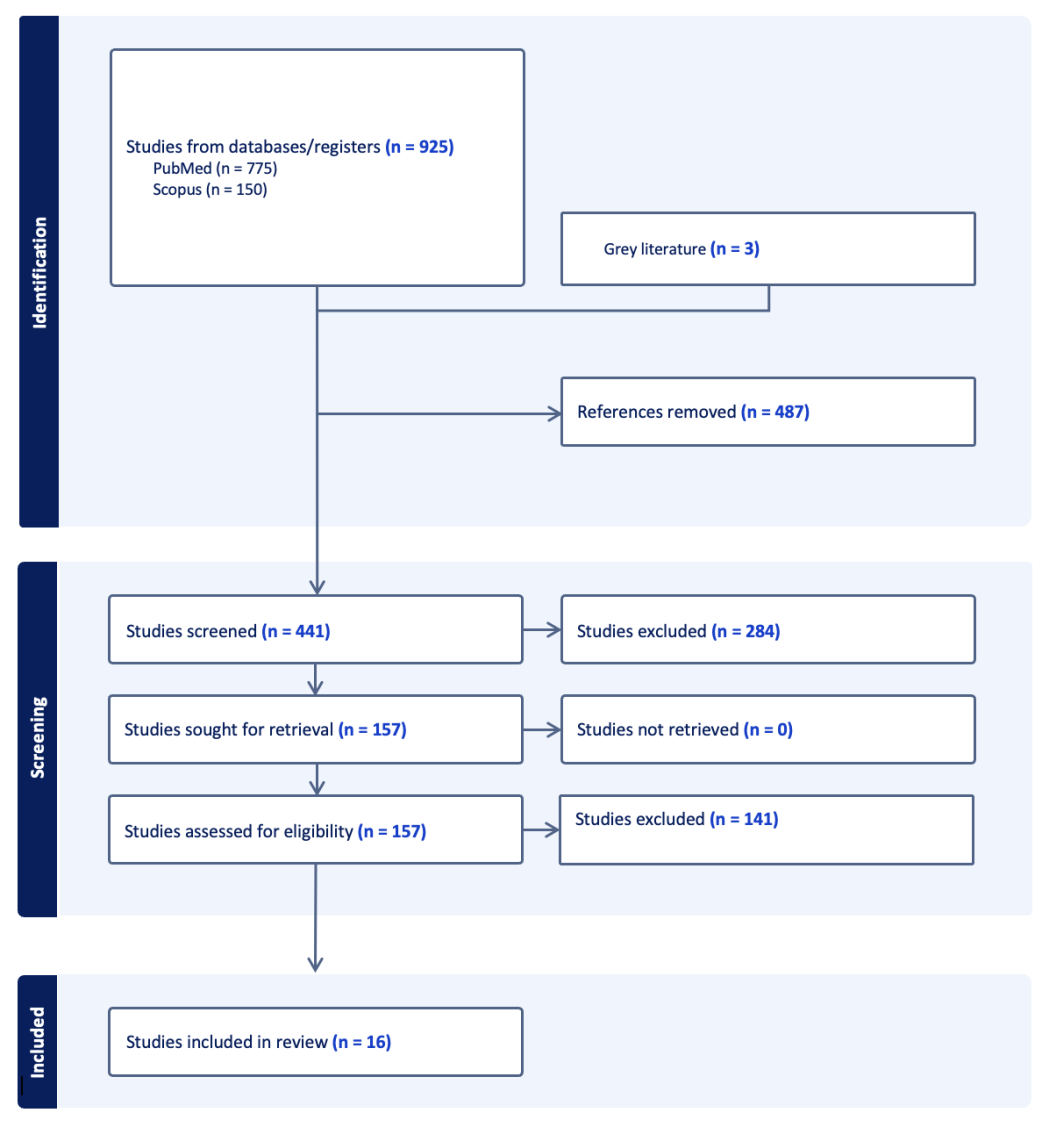
Scopus and PubMed Searches produced 925 results from 18 search combinations using 25 unique keywords. Within these results, 487 duplicates were identified, and three sources of grey literature were added, resulting in 441 unique articles. The 441 articles were screened in the title and abstract screening stage. Upon screening the tile and abstracts of the 441 studies, 284 were marked as irrelevant. The remaining 157 full-text articles were assessed for eligibility, and 16 were included in the review. A flow chart of this literature review can be seen in the appendix under Figure 3.
Additional parameters were developed while screening abstracts and full texts to keep a narrow focus on the research topic. Unlike Scopus, PubMed could not automatically exclude all systematic and literature reviews using a research type filter in the initial search. Many articles were excluded based on study design during screening abstracts and full texts in Covidence. Additionally, there is research surrounding the use of the ketogenic diet as a medical intervention for a variety of conditions; many were unrelated to the mental health conditions focused on in this research topic and were excluded after review.
Articles included a single-arm clinical trial, retrospective analysis, case studies, case- control studies, a cross-sectional study, an observational analytic study, a qualitative study, consensus guidelines, and a few peer-reviewed perspective articles. The articles included were from 2015 to 2024, with the majority published in the past five years, from 2019 to 2024.
Metabolic and Mental Health Outcomes
Because of the recent interest in this topic and the developing nature of this field, the literature review returned many studies focused on identifying both metabolic biomarkers and mental health outcomes of using metabolic ketogenic therapies for mental health conditions.15,19 Returned articles show positive results in pilot studies,15,19 case studies20-22, and case-control studies.23 A common theme from these articles was their aim to provide a greater understanding of how metabolic health and mental health are associated and how biomarkers and psychological measures change with the introduction of the ketogenic diet as a medical intervention.
Throughout the development of this critical analysis, results were published by Stanford Medicine in March 2024, the first U.S.-based clinical trial since 1965 to examine the therapeutic impact of a ketogenic dietary intervention for serious mental illness.19 The announcement of this study publication and its respective results represent a significant step forward in supporting the hypothesis that medical ketogenic therapies have improvements for participants in both metabolic health measures and psychiatric outcomes. Similar to the 2022 retrospective analysis conducted in France- The Ketogenic Diet for Refractory Mental Illness: A Retrospective Analysis of 31 Inpatients,15 the pilot trial conducted by Stanford Medicine titled Ketogenic Diet Intervention on Metabolic and Psychiatric Health in Bipolar and Schizophrenia: A Pilot Trial,19 shows the efficacy and feasibility of the ketogenic diet to improve both metabolic and psychiatric outcomes. Not only did the research team achieve significant results, but they implemented this regimen in an outpatient population, as opposed to the retrospective analysis, which was conducted on patients restricted to a psychiatric hospital.15,19
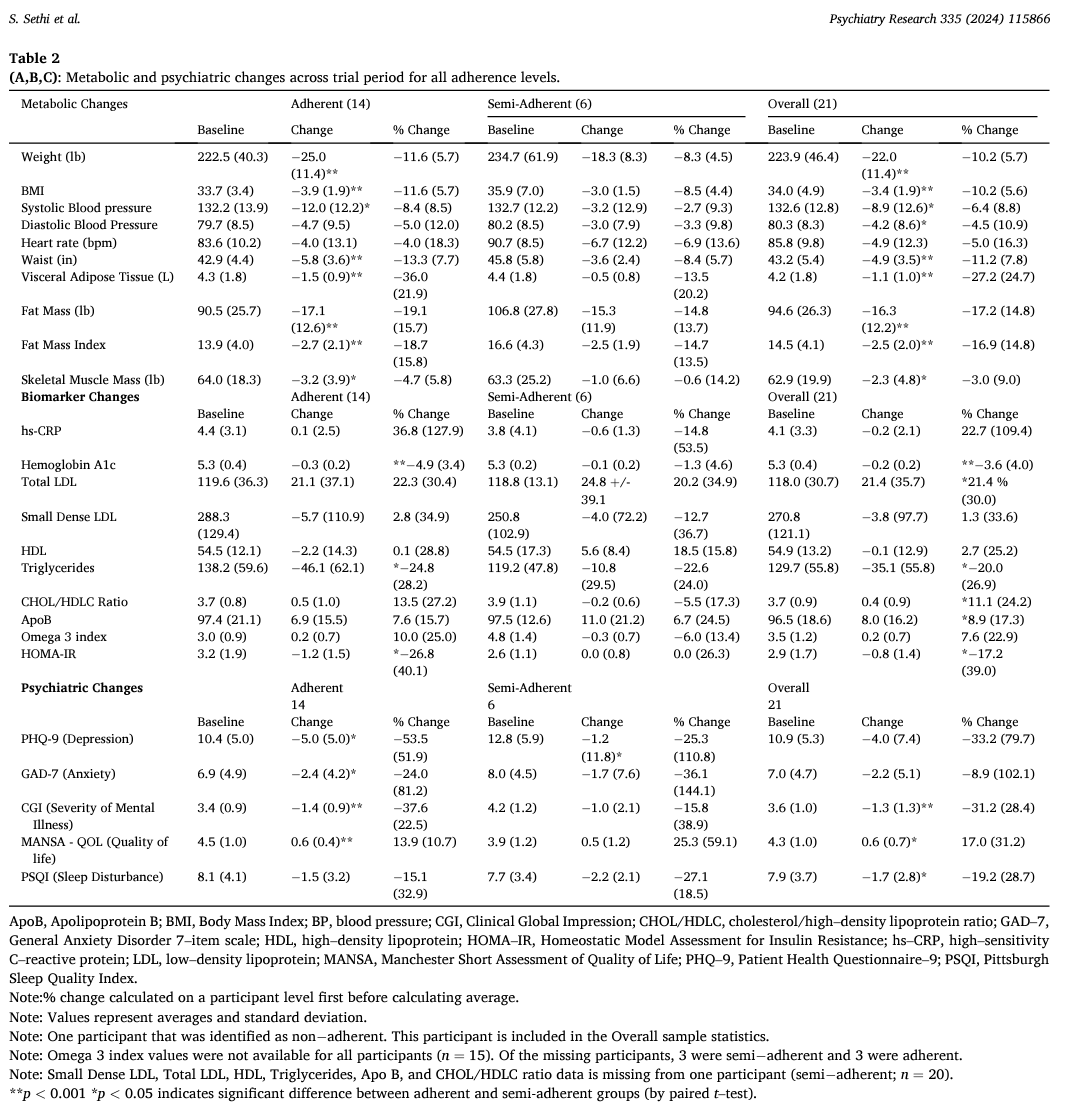
The study was a single-arm proof of concept study, testing a 4-month intervention of the ketogenic diet (10% carbohydrate, 30% protein, and 60% fat) for participants with a DSM-5 diagnosis of schizophrenia or bipolar disorder.19 Notable metabolic highlights include 100% of participants who were classified as having metabolic syndrome were in remission of their metabolic syndrome by the end of the study; the cohort experienced statistically significant measures of a 10% average reduction in weight, an 11% average decrease in waist circumference, a 17% average decrease in fat mass index, and an average visceral adipose tissue reduction of 27%.19 For psychiatric outcomes, an assessment of the severity of psychiatric symptoms was measured on Clinical Global Impression (CGI) scales.19 Clinically meaningful psychiatric improvement, measured by a 1-point change of more on the CGI scale, was shown in 79% of participants.19 On average, the severity of mental illness among the cohort improved by 31%.19 100% of participants who were “fully adherent,” defined as ketone measures >0.5 millimolar (mM) 80% of the time, achieved a recovered state, according to the Clinical Mood Monitoring definition.19 These results show a dose-response relationship between participants' adherence level and the strength of their psychiatric outcomes. This means that the closer the participants adhered to the intervention, the more significant results they achieved. The study also found improvements in other psychiatric outcomes, including an increase in life satisfaction, an enhancement in overall functioning, and an improvement in sleep quality.19 A detailed table of the trial's complete metabolic and psychiatric changes across the trial period for all adherence levels can be found in Figure 4 in the appendix.19 While this study conducted by the Stanford Metabolic Psychiatry Clinic was limited to a small group of participants (n=21) and lacked a control arm, the results demonstrate that a ketogenic diet intervention is a feasible and acceptable supplemental treatment in an outpatient setting, showing significant improvements in metabolic health measures and psychiatric outcomes for individuals with bipolar disorder and schizophrenia.19
The literature review highlighted many case studies on metabolic and mental health improvements.20-23 Harvard Medical School psychiatrist and author of Brain Energy, a book highlighting his research and experience in the metabolic mental health field, Chris Palmer, published two articles: case studies from 2017 and 2019 detailing his patients’ experiences.20,21 In two cases of schizoaffective disorder, both patients had a prior psychiatric history with medication history with more than ten medication treatment trials.20 They both experienced a dramatic decrease in psychiatric symptoms measured by the Positive and Negative Symptom Scale (PANSS) with their adoption of the ketogenic diet (patient 1 had a baseline score of 98 reduced to 49; patient 2 had a baseline score of 107 reduced to 70).20 Both patients also noted dramatic reductions in hallucinations and delusions, with increases in mood, energy, and their ability to concentrate.20 Metabolic outcomes were also found, with both patients losing a substantial amount of weight, a critical metabolic marker (patient one lost 104lbs, patient two lost 30lbs).20 Palmers 2019 publication described two cases of complete remission of psychotic symptoms in schizophrenia.21 The first case details an 82-year-old woman with a 65-year schizophrenia diagnosis, weighing 330 pounds and on a combination of 6 psychiatric medications before starting the ketogenic diet.21. Over a few months, while she continued the diet, she stopped all her medications as her hallucinations and paranoia remitted completely.21 She lost a total of 105 pounds, remained free of psychotic symptoms for 12 years, regained independence, no longer requires the care of a guardian or support from a PACT team, and reports she is happy to be alive.21 The second case showed a 39-year-old woman with a history of depression, anxiety, anorexia nervosa, and a 1993 schizophrenia diagnosis. Her psychotic and mood symptoms persisted despite 13 medication trials.21 The case described that within a month of starting a combination of the ketogenic diet along with the medication Haldol-decanoate, the woman reported complete remission of her psychotic symptoms for the first time since 1993, despite trying Haldol-decanoate in the past without a treatment response.21 She was tapered off Haldol-decanoate over the following year and has been off all antipsychotic medications for the past five years, lost 40 pounds, finished graduate school, and works a full-time job.21The results of Palmer’s case studies exemplify that, in some cases, ketogenic metabolic therapy can be used in the treatment and complete remission of schizophrenia. These findings also indicate that in some cases, the ketogenic diet, when monitored appropriately with the oversight of a trained provider, can be performed successfully in combination with medication;20 and, in some cases, patients have been able to taper off medications, continuing the ketogenic diet successfully, and have achieved complete remission of psychotic symptoms for 5 and 12 years.21
The literature review also returned another case study of a male patient who exhibited complete remission of bipolar disorder with the adoption of a ketogenic diet while increasing the intensity to achieve what is referred to as “depth of ketosis”.22 This study highlighted that in some cases, the depth of ketosis, or ketone level, correlates with patient outcomes.22 The patient in this case study experienced a complete absence of depression after eight years of chronic depression.22 The patient discontinued quetiapine from the pharmacological treatment and remained at a dose of 100 mg of lamotrigine without any symptoms of illness, depression, or hypomania.22 It is notable that the patient had unsuccessful attempts with lamotrigine before the adoption of the ketogenic diet, even in higher doses (300 mg/day).22 This case study stressed that the state of ketosis and its intensity (so-called depth) or increase in ketone level (mmol/liter) could determine the mood-stabilizing effect. In this regard, the author hypothesized that a tool to monitor the effectiveness of the ketogenic diet therapy might be the GKI coefficient (Glucose Ketone Index), which indicates the relation between the concentration of glucose and the ketone body β-hydroxybutyrate.22 This case study incorporated the suggestion that tools like the GKI coefficient to monitor the effectiveness of ketogenic metabolic therapies are needed to help patients and providers better understand how the depth of ketosis is correlated to mental health and metabolic health outcomes.
The literature review also returned a case-control study attempting to determine the energy demands of patients with schizophrenia.23 The authors gathered blood samples of 54 patients with schizophrenia and 54 control subjects.23 The authors found significantly higher serum levels of ketone body β-hydroxybutyrate in the patients with schizophrenia than in their age- and gender-matched healthy control subjects.23 These results suggested that there may be higher demands in energy utilization for patients with schizophrenia and may be an indicator of energy utilization impairment for schizophrenia.23 This analysis of schizophrenia patients and the differing energy demands opposed to healthy control subjects warrant further research into brain metabolism and the relationship between serum levels of ketone body β-hydroxybutyrate and energy utilization impairment for schizophrenia.
Future Feasibility
Due to the explosion of interest in this topic, results were returned on the feasibility of using the ketogenic diet in the prevention, management, and treatment of bipolar disorder, major depression, and schizophrenia .24,25
A 2023 pilot study of a ketogenic diet in bipolar disorder assessed the recruitment and feasibility of conducting the ketogenic diet as an intervention for bipolar disorder.24 Researchers recruited and enrolled 26 patients, 20 of whom completed the modified ketogenic diet for 6-8 weeks.24 With 91% of all readings indicating ketosis, a high degree of adherence to the diet was suggested. This evidence shows that it is feasible to recruit and retain individuals with bipolar disorder who maintain ketosis and have a high degree of completion rates. Therefore, this study proves to be a base for warranting future randomized control trials to test ketogenic metabolic therapies for bipolar disorder.
The literature review also returned a protocol for a randomized control trial that was published in April 2024 out of the University of Oxford to evaluate the efficacy and mechanisms of a ketogenic diet as an adjunctive treatment for people with treatment-resistant depression.25 One-third of people with depression do not respond to antidepressants and, after two adequate courses of antidepressants, are classified as having treatment-resistant depression (TRD).25 This study aims to become the first randomized, controlled trial assessing the effects of a ketogenic diet on symptoms of depression in patients with treatment-resistant depression. Researchers will measure participants’ scores on the Patient Health Questionnaire (PHQ-9) from baseline to 6 weeks using a placebo intervention group and a ketogenic diet group.25 The protocol calls for both groups to receive nutritional support with weekly 30-minute dietician counseling sessions.25 The publication of this protocol is a foundation for the first randomized control trial to test whether a ketogenic diet is an effective intervention to reduce the severity of depression, anxiety, and improve quality of life and functioning ability for people with treatment-resistant depression.25 If this study produces results similar to The Ketogenic Diet for Refractory Mental Illness: A Retrospective Analysis of 31 Inpatients19, and the Stanford Medicine pilot trial titled Ketogenic Diet Intervention on Metabolic and Psychiatric Health in Bipolar and Schizophrenia: A Pilot Trial,20 there will be substantial evidence supporting positive outcomes in both metabolic and mental health outcomes.
Dietary Adherence, Family Support, and Education Programs
The restrictive nature of limiting carbohydrates in a ketogenic diet can be challenging for patients. As seen by the results in the Stanford pilot trial,20 the retrospective analysis,19 and the depth of ketosis case study,22 dietary adherence is a crucial factor in the effectiveness of the diet to produce desired mental health and metabolic outcomes. Because of the precedence of effective use of the ketogenic diet in other conditions, articles were included based on the relevancy of specific tools and programs that would also be applicable for the use in supporting ketogenic metabolic therapies targeting serious mental illness.
The ketogenic diet is the gold standard treatment for glucose transporter type 1 deficiency syndrome (GLUT1DS), a rare neurological disorder.26 A case study report was conducted to investigate the effectiveness of a psychoeducational program named “KETOLAND” implemented partially through telepsychology, based on Cognitive Behavioral Play Therapy (CBPT) to support ketogenic dietary therapy knowledge and adherence for a GLUT1DS patient and her supporting family.26 The case study noted that adoption of a ketogenic diet could be challenging for patients and their families, with meal preparation being “extremely demanding”.26 Through ten weekly meetings with the patient and her family, a multidisciplinary team of a neurologist, psychologist, and dietician used therapeutic storytelling through the creation of an educational booklet entitled “Ketolandia: in search of the ketone door.”26 The “KETOLAND” psychoeducational program resulted in an increase in knowledge for the patient and her family, along with telepsychology access to her team, which led to better dietary adherence.26 The results from this study indicate that creating standardized tools to detect ketogenic dietary therapy knowledge and adherence would be helpful for clinical purposes.26 The study also noted the telepsychology delivery model as a sustainable way of overcoming the distance and cost barriers to health care delivery, as well as reporting the patient and her family are more comfortable being at home in their own house, viewing the education as a support to their daily lives.26
The search also found a pilot randomized trial to improve adherence to a Mediterranean Ketogenic Nutrition Program (MKNP), which was seen to achieve higher adherence using the Health Obesity-Related Behavioral Intervention Trials (NIH ORBIT) model to develop and pilot a program to help older adults with memory concerns use the Mediterranean Ketogenic Nutrition.27 Motivational interviewing (MI) strategies and behavior change techniques (BCT) were used only in the Mediterranean Ketogenic Nutrition arm, in which the group reported higher objective and self-reported adherence.27 The results from this study suggest that incorporating MI and BCT strategies may better engage and retain participants than a nutrition education program alone.
Adherence questionnaires were also identified as a valid tool to improve adherence. The literature review returned two studies that used factor analysis to validate questionnaires for adherence to ketogenic dietary therapy.28,29 The Brazilian questionnaire “Keto-check,”28 and the Italian questionnaire “iKetoCheck,”29 were both concluded to be valid tools for evaluating KDT adherence, which patients, families, and clinicians can use to improve patient management and optimize the effectiveness of KDT’s.
To support dietary adherence, the 2024 Stanford Medicine pilot trial for bipolar and schizophrenia included access to health coaches in their 4-month intervention.19 Participants could reach out to their health coaches as needed to support them throughout the study.19 On average, health coaches checked in with the individuals enrolled in the study for 5-10 minutes per week throughout the study.19 Additionally, the Oxford study's proof-of-concept randomized control trial protocol will provide participants with pre-prepared ketogenic diet meals (3 meals per day) and snacks to support adherence.25 Like the Stanford Medicine pilot trial, the Oxford depression study aims to measure adherence as an exploratory study objective.25
Questionnaires, Screening, and Assessment Tools- 65
The studies included in the literature used a variety of assessments, scales, and medical equipment to screen and measure psychiatric and metabolic outcomes. Common metabolic measures were recorded across multiple studies, including vital signs such as heart rate, blood pressure, height, weight, waist circumference, and body composition measurements.15,19,20,21,22 Bloodwork samples were tested to conduct a more detailed metabolic panel to measure insulin resistance and other metabolic health factors,19 and to determine the serum levels of ketone body β-hydroxybutyrate.23 Ketone measurements were measured by urine ketone monitoring,15 and blood ketone levels were measured with a blood ketone meter.19 Depth of ketosis was measured using the GKI coefficient (Glucose Ketone Index).22
Psychiatric assessments were conducted in both the studies and case reports to understand changes in mental health symptoms. To measure depression, the Patient Health Questionnaire Depression Scale (PHQ–9) was used to assess depression metrics at baseline and different points throughout the study.19, 25 In the retrospective analysis of 31 inpatients, refractory depression symptoms were measured by the Hamilton Depression Rating Scale (HAM-D) and the Montgomery-Åsberg Depression Rating Scale (MADRS).15 Changes in illness severity were measured by the Clinical Global Impressions Scale (CGI-S),15 Clinical Global Impression– Schizophrenia (CGI–SCH),19 and Clinical Global Impression for Bipolar Disorder–Overall Severity (CGI–BP–OS).19 The Positive and Negative Syndrome Scale (PANSS) was used to measure changes in psychosis symptoms in the retrospective analysis,15 and the case studies by Dr. Palmer.20,21 PANSS was also used to assess the disease characteristics and psychopathology of patients with schizophrenia in the ketone body case-control study.23
Other notable outcomes measured were sleep quality based on the Pittsburgh Sleep Quality Index (PSQI),19 screening, and evaluation of potential side effects associated with the KD conducted by clinicians’ clinical visits,19 and quality of life assessments Manchester Short Assessment of Quality of Life (MANSA).19
Introducing A Public Health Framework
The research surrounding serious mental illnesses, MDD, BP, schizophrenia, and the relationship to metabolic health using ketogenic metabolic therapies has shown promise to treat and maintain symptoms, allowing for a better quality of life for individuals and their families. A comprehensive framework is needed for adapting this innovative approach to healthcare settings to support the population health of the 11% of U.S. adults who struggle with MDD, BP, and schizophrenia.3,5,7
To achieve population-level impact, many factors need to work together concurrently to mitigate the effects these serious mental illnesses have on a vulnerable population. Due to ketogenic dietary therapies requiring a substantial behavior change, support is needed for individuals, education is necessary for their relationships, positive change needs to be supported by community efforts, and society needs to understand and adopt positive practices to support implementation. The Social-Ecologic Model can be used as a public health framework for integrating ketogenic metabolic therapies in the prevention, interventions, and management of MDD, BD, and schizophrenia. A balanced and sustainable public health approach can be achieved by implementing programs, policies, and systems that support each level of individual, relationship, community, and societal factors.
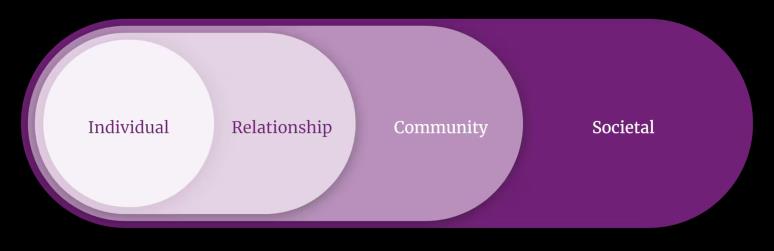
Individual- Biological and personal history factors are correlated with an individual’s chance of having a serious mental illness.15,19 A family history of mental illness, a history of traumatic events, and alcohol and drug abuse are all risk factors for MDD, BP, and schizophrenia.4,6,8 We now know that metabolic and mental health are interconnected. More research connecting metabolic health to mental health continues to draw correlations. During the development of this critical analysis, new results from a population-based cohort study were published in April 2024 by the JAMA Network.30 The population-based cohort study with longitudinal data collection assessed 211,200 participants from the Apolipoprotein-Related Mortality Risk (AMORIS) cohort from an occupational health screening beginning in 1985 in Sweden.30 With a mean follow-up of 21 years, 16,256 individuals were diagnosed with depression, anxiety, or stress-related disorders.30 The case-control analysis concluded that individuals with biomarkers showing high levels of glucose and triglycerides and low levels of high-density lipoprotein were associated with an increased subsequent risk of all tested psychiatric disorders.30 This longitudinal data collection of more than 200,000 individuals means that the metabolic health of individuals, shown by biomarkers of carbohydrate, lipid, and apolipoprotein metabolism, is associated with an increased risk of depression, anxiety, and stress-related disorders. Therefore, education programs that promote self-efficacy for individuals who are at risk for serious mental illness are necessary to allow individuals to take control of their health. By practicing habits that are conducive to achieving and maintaining strong metabolic health, individuals can decrease their risk of serious mental illness. By equipping individuals with the knowledge and tools to take care of their health by making positive food choices, prioritizing consistent sleep, and participating in regular exercise, individuals can be empowered to make behavior changes, aiding in the prevention of serious mental illnesses.
Relationship- The U.S. healthcare system is constructed in a way where individuals only interact with the healthcare system when they need care. It is a reactive model with individuals spending more than 99% of their time outside of the healthcare system, left to make their own decisions daily, which impact physical and mental health. Patients' relationships with their medical providers are a crucial part of their health care. Primary care providers often serve as patients' first line of interaction with the medical system. Patients need to be able to interact with their team of providers and trust that the providers are well-equipped with the most up-to-date tools. This is why training clinicians with the most up-to-date modalities is a critical part of integrating ketogenic metabolic therapies and using programs that support prevention, management, and adherence to the diet. Reaching primary care providers to educate them on how metabolism is part of the mental health process and how important it is to target both metabolism and mental health outcomes. Primary care providers need to be equipped to recognize risk factors for serious mental illness and know when to deploy screening tools and possible interventions to mitigate risks. Mental health clinicians, as both prescribers and psychotherapists, need to be trained on the nuances of ketogenic metabolic therapies and potential side effects so they can tailor their treatment toward individual needs. Patients need to feel comfortable having access to providers as they are going through a substantial lifestyle change.
While more research continues, large hospital systems move slowly and often need to see large, robust, randomized clinical trials, which, while underway,18 take years. Therefore, it is essential to train and educate providers so they can help patients. There are psychiatrists, psychotherapists, mental health counselors, dieticians, and health coaches who are gaining insights by utilizing ketogenic metabolic therapies in practice.31 The practical, real-world challenges of transitioning from research to clinical experience are essential to understand, and the early adopters of this intervention possess valuable experience and viewpoints of best practices that need to be disseminated. Establishing continuing medical education (CME) courses to train clinicians would further guide and equip providers with the necessary knowledge to serve patients who may benefit from ketogenic metabolic therapies. By establishing CME courses for a variety of mental health specialties, clinicians can be trained to recognize when and who may benefit from ketogenic metabolic therapies.
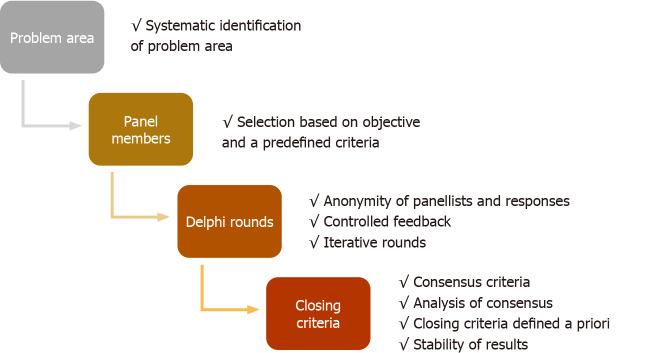
Consensus guidelines for using the ketogenic diet as a dietary intervention for epilepsy were published by experts in the field in 2009 and updated in 2018.32 These guidelines provided a structured, evidence-based practice for dieticians and other medical providers to refer to when using ketogenic therapy specific to epilepsy.32 For the use of ketogenic metabolic therapies specific to mental illness, consensus guidelines should be developed and updated by experts in the field. Consensus guidelines can be developed using a “Delphi Method.” This method synthesizes a consensus or saturation of results from questionnaires sent to clinicians using the therapeutic procedure. The questions are created by a multi-disciplinary team of experts in the field, sent to clinicians, and then reformulated until participants agree upon a well-established consensus.33 The results are then submitted as consensus guidelines for publication in medical journals. A visual representation of the Delphi Method can be seen in Figure 6.33
Integrating the ketogenic diet as a dietary intervention involves a substantial behavior change, which is why incorporating health coaches on a multidisciplinary treatment team is a great idea to expand the mental health workforce. Access health coaches were seen to be effective in the Stanford Medicine pilot trial even in a small amount of time, 5-10 minutes per week.19 Additional dietary support can aid patients in understanding which foods to choose, how to prepare them, and a therapeutic approach for understanding the patient’s relationship with food; all necessary support will increase adherence to the intervention. Policy upgrades should be made to allow insurance billing for certified health coaches, improving access and affordability for patients to benefit from this additional supportive relationship.
Creating standardized tools to detect ketogenic dietary therapy knowledge and adherence would be helpful for patients and families. Education programs like the psychoeducational program seen in the KETOLAND study26 build family education and support, leading to adherence. Clinicians have stated that patients report that cultural traditions and peer pressure can make restricting carbohydrates challenging.31 By building a patient's self-efficacy and educating their inner circle, patients can advocate for themselves and receive support from their immediate relationships to nurture their metabolic and mental health.
Community- Improving the physical and social environment of community settings is critical to supporting individuals at risk for serious mental illness. Schools, workplaces, and neighborhoods are all places in which social interactions take place. Leadership from local government, entrepreneurs, school boards, and community groups is needed to make the places where people live, learn, work, and play conducive to behaviors that support health. There is an opportunity to educate the public on the metabolic mental health connection and the behaviors they can take to help their well-being and the health of their neighbors.
By having employers, school leaders, and primary care providers take an evolved view of mental health by screening for metabolic biomarkers along with the traditional psychiatric screening tools, there can be earlier detection of insulin resistance and metabolic syndrome to understand populations at risk for serious mental illness. Local government can take measures to improve access to grocery stores, encourage farmers’ markets, create community programs to promote exercising and eating healthy and reduce ultra-processed foods in school lunches. Encouraging people to use tax-advantaged healthy savings accounts (HSA) and flexible savings accounts (FSA) to make purchases to prevent diseases should be promoted and educated to the public. People do not traditionally think of using HSA/FSA accounts to purchase supplements, wearable health devices, and exercise services to prevent, manage, or reverse diseases. Still, many health products and services are possible with letters of medical necessity. To foster community and a sense of identity, in-person support groups, and virtual groups via social media and internet platforms should be created for those maintaining a ketogenic diet. This will increase the sense of community and accountability, likely resolving in greater adherence.
Societal- In recent months, news and publications about this topic have reached mainstream media attention. From news coverings on NPR, The Today Show, and some of the world’s largest podcasting platforms to industry-leading magazines and publications like Psychology Today and Medscape, researchers and advocates are having their voices and results heard. Advocacy groups and non-profit organizations such as Metabolic Mind are now distributing videos, podcasts, blog articles, and free resources for individuals and families to seek help. This continued dissemination of information is vital to get the message out to the public of a new and viable treatment option for people who have struggled to find success with traditional therapies. Continued mass public health communications should also point to the connection between metabolic and mental health and describe how important it is for Americans to care for both and engage in preventative measures like making informed food choices, prioritizing sleep, and sustainable consistent exercise.
To ensure proper delivery and sustainability of a long-term shift in mental health prevention, management, and treatment, focusing on quality food, we must zoom out and think about the health of our food systems. The dominant breakdown of this diet comes from protein and fats (10% carbohydrate, 30% protein, and 60% fat).19 Our current food system needs to be equipped to handle an increase in demand for at least the 11% of our U.S. adult population who may benefit from a shift towards eating this way. Changes in the USDA Farm Bill will be necessary to support an evolved approach connecting our food to our metabolic and mental health.
The health of our environment, the quality of our nutrients, the sustainability of our food system, and our reliance on other countries to import specific foods are all critical factors that can be impacted by policy and a societal shift in attitude toward the importance of this and how it relates to both metabolic and mental health. Policies promoting crop rotations and regenerative agriculture would revitalize our soil and sequester carbon from the atmosphere while producing more nutrient-dense fruits, vegetables, and livestock. By transitioning from industrial monocropping to regenerative agriculture, we would reduce our reliance on and consumption of environmental and human toxins like herbicides and pesticides.
Societal changes in public policy may seem far away or too early to think about. However, it is essential to be ready and understand the implications of a significant shift in mental health care delivery. Tools like blood glucose and ketone testing meters improve accuracy and support adherence and should be fully integrated with health insurance plans and covered devices on the Medicare and Medicaid formulary. Suppose future randomized control trials or an overwhelming amount of case studies show that a dietary intervention consisting of a varied ratio of macronutrients (10% carbohydrate, 30% protein, and 60% fat) is as or more effective than psychiatric drugs. How can we as a society continue to allow reimbursement from insurance for pharmaceuticals and not for the specific ratio of macronutrients? Will we see patented “Keto meals”? Will all kinds of fats like grass-fed butter and soybean oil be treated the same way, or will only those deemed medically healthier or practical for someone following this diet be approved? And who is the person or agency making that call? Do they have any conflicts of interest? These are all future policy questions that must be delicately handled to ensure the integrity remains intact and that a new way to prevent, manage, and treat metabolic and mental health remains intact.
Discussion
The implications of the findings in this literature review closely link metabolic health to mental health and exhibit great hope for public health, garnering further exploration and development in preparation for what will need substantial changes to adapt to a new prevention and care model. A strength of the literature review was the precedence for the programs, screening tools, and adherence tools, which can be replicated and modified for use when using the ketogenic diet for mental health. Limitations of the review are that the study was not limited to the U.S. population, limiting the complete application of the findings and tools found. Additionally, few clinical trial studies specifically focused on major depression, bipolar disorder, and schizophrenia. Although protocols have been developed, because of the nascent nature of this topic, a limitation is the lack of robust clinical trials and the limited programs, tools, and education explicitly developed for major depression, bipolar disorder, and schizophrenia.
We are nearing what could be a turning point in the public perception of mental health prevention and treatments. This is a point where deeper research has begun, and communication has started about the significant mental health and metabolic improvements used by implementing a ketogenic diet. Shifting the brain’s energy source from glucose to ketones can have considerable metabolic and mental health outcomes for individuals. Through adherence tools, improved education, and programming, families, providers, and patients can enhance their relationships with each other. We can foster an environment conducive to positive behavior change as a community. Finally, as a society, we can shift our view and support long-term policies to give more possibilities and hope to a population that has struggled so much for far too long.
Appendix
Ketogenic Diet
Figures
This is a self-published version of my Master of Public Health thesis. The complete document, including all references, is available in the full PDF.